
2025-11-04
The patient, in his prime years, enjoys a happy family and successful career. He presented with right lower limb pain. Examinations revealed osteolytic destruction of the L4 vertebral body, and his Prostate-Specific Antigen (PSA) was significantly elevated. After seeking multiple opinions, he consulted Dr. Han Liangfu from the Foshan Chancheng Hospital Tumor Precision Diagnosis and Treatment Center's Prostate Cancer Multidisciplinary Team (MDT). Further workup, including a whole-body PET/CT scan and a prostate biopsy, confirmed the diagnosis: Prostate Cancer with an isolated bone metastasis to the L4 vertebra.

Director Han Liangfu reviewing the patient's medical records.
For a patient with advanced, metastatic prostate cancer, surgery is no longer the primary treatment option. Determining the overall treatment strategy—to both alleviate the limb pain symptoms and preserve limb function, while also achieving the goal of cure through local precision therapy based on comprehensive systemic treatment—became the paramount focus of this case.
01 Case Presentation
Male, 57 years old.
Clinical Diagnosis: Low-Volume (Oligo) Metastatic Castration-Sensitive Prostate Cancer, cT2bN0M1b, Stage IVB.
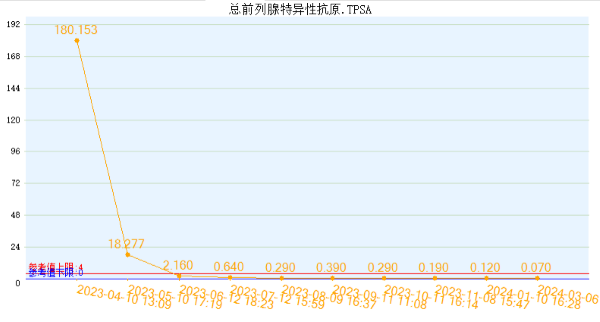
PSA: 180.153 ng/ml.
Gleason Score: 4+4=8.
02 History and Diagnosis
2023/4
The patient experienced "right lower limb pain" for 1 month. Initial PSA: 139 ng/ml. Contrast-enhanced lumbar spine MRI showed: osteolytic destruction of the L4 vertebral body and right appendage with soft tissue mass formation, highly suggestive of malignant bone tumor or metastatic tumor. The patient occasionally felt difficulty urinating, but no frequency, urgency, dysuria, or increased nocturia.
2023/4/6
Repeat PSA: 180.153 ng/ml;
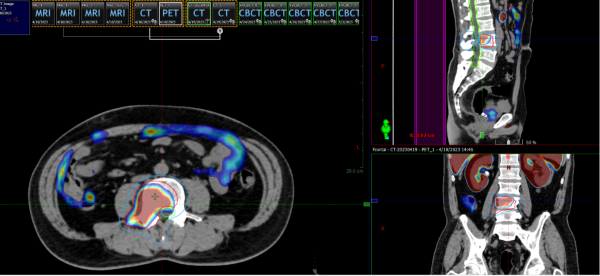
FDG and PSMA-PET/CT Whole-Body Scan:
Heterogeneous increased 18F-PSMA uptake within the prostate. PSMA-PET showed multiple nodular and patchy areas of increased radiotracer uptake in the prostate, the largest located in the left lobe (1.9*2.9 cm, SUVmax 9.2), consistent with prostate cancer.
Metastasis to the L4 vertebral body and right appendage, showing significantly increased radiotracer uptake, SUVmax 13.5.
2023/4/10
Contrast-enhanced MRI: Enlarged prostate volume (approx. 55.7*40*44.1 mm). Abnormal signals in bilateral peripheral zones, the larger one in the left peripheral zone (approx. 12 mm diameter), showing slightly high signal on DWI with mild diffusion restriction, low signal on ADC, and heterogeneous enhancement post-contrast, consistent with prostate cancer. No enlarged pelvic lymph nodes. Patchy low signal in L4 vertebral body and right appendage, showing enhancement.
2023/4/11
Ultrasound-guided prostate biopsy with concurrent fiducial marker placement.
Post-operative Pathology:
(Left Base) Prostatic acinar adenocarcinoma, Gleason Score 4+4=8, ISUP Grade Group 4, cancer comprises 40% of the core, no lymphovascular or perineural invasion; P504S+, P63-, PMS2+.
(Right Base) Prostatic acinar adenocarcinoma, Gleason Score 4+4=8, ISUP Grade Group 4, cancer comprises 5% of the core, no lymphovascular or perineural invasion; P504S+, P63-.
(Left Apex, Left Mid, Right Mid, Right Apex) show benign prostatic hyperplasia.
03 Treatment Course
A middle-aged male, newly diagnosed with prostate cancer and an isolated L4 vertebral bone metastasis. Following an International Multidisciplinary Team (MDT) discussion involving the Foshan Chancheng Hospital Tumor Center expert team and international experts like Professor Dr. Dian Wang from the Department of Radiation Oncology, RUSH University Medical Center, USA, the overall treatment decision was long-term (2-3 years) Androgen Deprivation Therapy (ADT) combined with local precision radiotherapy (SBRT) to both the primary prostate cancer and the L4 bone metastasis.
Treatment Goals: ① Strive for long-term survival and potential cure; ② Alleviate pain symptoms and improve quality of life.

International Multidisciplinary Team (MDT) Discussion
2023/4/14
The patient started ADT (Goserelin 3.6mg subcutaneously every 4 weeks) + Bicalutamide oral therapy. Concurrently, Zoledronic Acid was administered for bone protection.
2023/4/24 - 5/3
Underwent Linear Accelerator-based SBRT to the L4 bone metastasis: GTV 8Gy5 fractions, concurrently CTV 6Gy5 fractions.
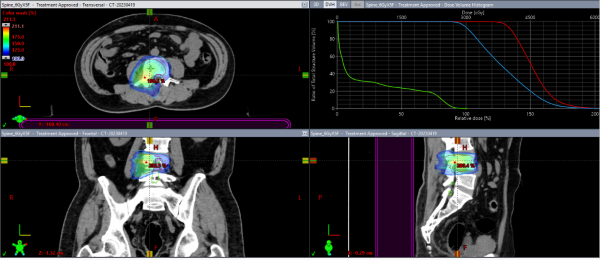
The patient's right lower limb pain significantly improved after radiotherapy.
2023/6/12 - 6/21
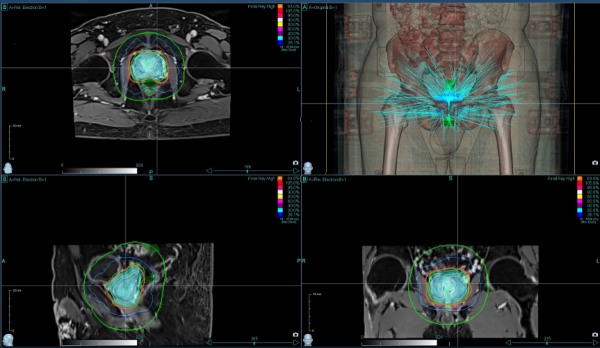
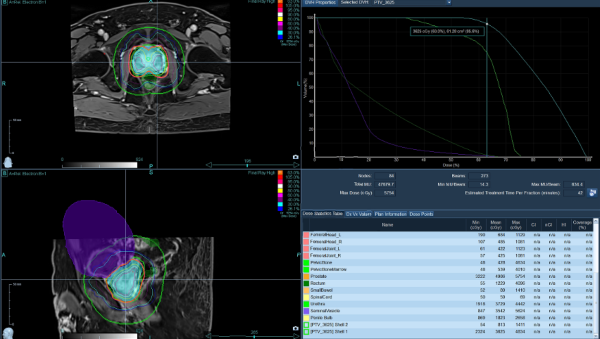
Underwent CyberKnife SBRT to the primary prostate lesion using dose-painting techniques and fiducial marker tracking: 7.25Gy*5 fractions.
The patient has continued monthly ADT (Goserelin 3.6mg) injections since completing radiotherapy.
Tolerance to all treatments was good, with no significant adverse effects reported.
04 Treatment Outcome and Follow-up
Post-treatment, the patient's right lower limb pain completely resolved. No significant intestinal or urinary side effects occurred following ADT and radiotherapy. The patient's mental state is excellent, and his life and work have returned to normal!
Serial PSA checks show a dramatic drop from the peak of 180.153 ng/ml. The most recent result is 0.07 ng/ml, representing a decrease of over 2500-fold!
05 Discussion
For metastatic prostate cancer, is local radiotherapy to the primary prostate and metastatic lesions necessary, in addition to ADT + anti-androgen therapy?
Current consensus indicates that local radiotherapy improves overall survival (OS) in prostate cancer patients with low metastatic burden (defined as fewer than 4 metastases, confined to axial skeleton, and no visceral metastases).
STAMPEDE Clinical Trial Subgroup Analysis: Among 1932 M1 patients, radiotherapy to the primary prostate tumor improved 3-year OS by 10% (85% vs 75%) in patients with up to 3 bone metastases, but showed no improvement in 3-year OS (52% vs 53%) for those with more than 4 bone metastases.
Reference: Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomized controlled phase 3 trial. Lancet 2018; 392: 2353–66
The treatment outcome in this case report strongly demonstrates the excellent short-term efficacy achieved by combining ADT with SBRT radiotherapy targeting both the primary prostate lesion and the isolated bone metastasis.
We will continue to follow the patient for long-term efficacy and side effects, hoping he can achieve a complete cure.

The Foshan CyberKnife system preparing for treatment.
06 M6 CyberKnife Technical Highlights:
◆ High Precision of CyberKnife Radiotherapy: 0.06mm treatment precision ensures accurate targeting, reducing side effects to the bladder and rectum, and preserving the patient's quality of life.
◆ Localized SBRT for Prostate: In the absence of pelvic lymph node metastasis, focused stereotactic CyberKnife radiotherapy to the prostate offers a shorter treatment duration (5 days) with manageable toxicity, leading to its increasingly widespread clinical application.
◆ Importance of Comprehensive Post-Treatment Management: Ongoing management after prostate cancer treatment is crucial. This involves ensuring patient adherence to medication schedules and long-term monitoring for disease recurrence and treatment-related side effects, allowing for timely intervention.


